By: Thalia Kaylyn Averil
Percutaneous Endoscopic Gastrostomy (PEG) is a method used to insert a feeding tube or what is called a PEG tube. This tube allows nutrients to be administered directly into the stomach. PEG is the method of choice for long-term enteral nutrition in patients with a functioning digestive system. The main goal of enteral and parenteral nutrition is to provide nutrients to patients who cannot consume enough nutrition orally, so their metabolic needs can still be met. Enteral feeding is administered through the gastrointestinal tract, while parenteral feeding is administered through the bloodstream. In general, enteral nutrition is better than parenteral nutrition in patients with a functioning digestive system because it is more similar to a normal digestive system. Therefore, enteral nutrition carries lower risks, lower costs, and is able to provide gut stimulation, which helps maintain the defense system in the intestines. In addition, administering enteral nutrition, especially through the stomach, has been shown to reduce the risk of bacteria transferring from the digestive tract to other parts of the body, such as the blood vessels or lymphatics.
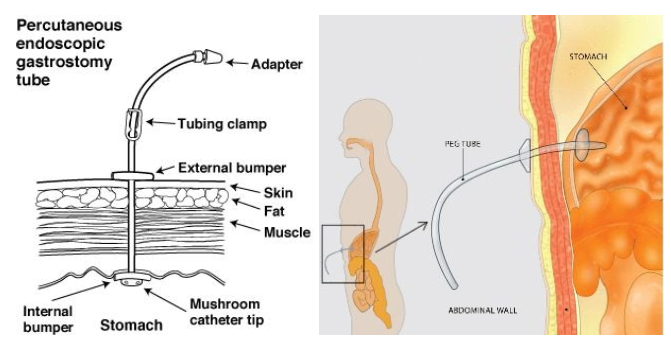
Figure 1. Percutaneous Endoscopic Gastrostomy (PEG).
PEG is primarily indicated for enteral feeding and gastric decompression. The most common type of enteral feeding is insertion of a tube through the stomach. Tube installation can be done using endoscopy, radiology, open surgery, or laparoscopy. In PEG, tube placement using endoscopic methods is preferred over surgical methods because it is less invasive and often does not require general anesthesia. PEG is currently the method of choice for enteral feeding for medium to long-term use.
PEG may be indicated if you experience dysphagia or difficulty swallowing which can be caused by various conditions such as brain injury, head and neck cancer, stroke, or loss of appetite due to diseases such as cancer. In addition, PEG can also be beneficial for individuals with conditions that can affect how their bodies process nutrients, such as patients with cystic fibrosis or kidney failure requiring dialysis. In some cases, comatose patients may use PEG to help maintain their nutrition and hydration.
One of the contraindications for PEG tube placement is a coagulation disorder that can lead to bleeding or blockage in the blood vessels. Another contraindication is hemodynamic instability, which includes blood pressure, heart rate, respiratory rate, respiratory rhythm, body temperature, and others. Moreover, patients with an infection in the abdominal wall, obstruction in the gastric outlet, history of total gastrectomy, gastroparesis causing the stomach to empty its contents abnormally, and peritoneal carcinomatosis should not undergo the PEG procedure. PEG is also contraindicated in patients with sepsis leading to widespread systemic inflammation and severe ascites or fluid accumulation in the abdominal cavity.
Patients undergoing PEG tube placement will fast for eight hours before the procedure and receive antibiotics as prophylaxis to prevent infection one hour before the procedure. There are several techniques used to insert the PEG tube, including the pull technique, push technique or guide wire technique, and the introducer method or Russell technique. Currently, the pull technique is the most commonly used technique for PEG tube placement. Most healthcare providers insert PEG tubes using an endoscopic method that utilizes a flexible instrument called an endoscope. During the procedure, the doctor makes a small incision in the upper abdomen, inserts the tube through the incision, and connects it to the stomach. Patients may receive a local anesthetic injection around the incision site.
The entire PEG tube placement procedure likely only takes between 20 to 30 minutes, and patients can go home the same day or the next morning. After the procedure, patients may experience mild discomfort, which could be due to the incision or cramping from gas buildup in the digestive system. This discomfort will usually disappear within 24 to 48 hours. In general, feeding is delayed until the next day or one to six hours after PEG placement because there is a higher risk of peritoneal leakage after feeding. To prevent tube blockage, the tube should be flushed before and after each administration of food and medication. In addition, medicines should be dissolved in water before administration and it is better to use medicines in liquid form rather than solid form to reduce the risk of tube blockage.
Resources
- Rahnemai-Azar AA, Rahnemaiazar AA, Naghshizadian R, Kurtz A, Farkas DT. Percutaneous endoscopic gastrostomy: indications, technique, complications and management. World J Gastroenterol. 2014 Jun 28;20(24):7739-51. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4069302/
- Cleveland Clinic. Percutaneous endoscopic gastrostomy (PEG) [Internet]. Cleveland: Cleveland Clinic; date of publication unknown [reviewed 2021 Apr 19] [cited 2024 Mar 19]. Available from: https://my.clevelandclinic.org/health/treatments/4911-percutaneous-endoscopic-gastrostomy-peg
- Gastroenterology Associates. Understanding percutaneous endoscopic gastrostomy [Internet]. Hagerstown: Gastroenterology Associates; date of publication unknown [cited 2024 Mar 19]. Available from: https://www.gidoc.biz/articles/asge_education_library/553774-understanding-percutaneous-endoscopic-gastrostomy/