By: dr. Sigit Pramono, Sp.OG, FRANZCOG

Introduction
Every gynaecologist remembers the first time they opened a large cervical fibroid. The plan always sounds straightforward in clinic. In theatre, it rarely is. The bladder sits forward, the ureters are dragged medially, and the uterine vessels disappear into a mass that has quietly rewritten the pelvic anatomy.
Cervical fibroids account for roughly 0.6% of all uterine leiomyomas.1 Because of this rarity, most trainees finish their training having seen only a handful. When they do appear, they behave badly. They distort the cervical canal, displace ureters, and make conventional myomectomy hazardous, with real risk of haemorrhage and urinary tract injury.1,2
The challenge sharpens when the patient is young and wants to conceive. Hysterectomy ends the conversation. Cervical myomectomy keeps the uterus but may leave the woman with a damaged, incompetent cervix. Medical therapy rarely shrinks a fibroid of this size enough to matter. This is the clinical space where High Intensity Focused Ultrasound (HIFU) has quietly become a credible option.3,4
Case Presentation
Mrs PS, a 29-year-old woman, presented with a six- to eight-month history of progressively increasing abdominal girth and dull lower abdominal discomfort. She had been trying to conceive for four years. Deep dyspareunia had become a regular feature of her married life. Her menses remained regular, lasting four to six days, with four to five pads per day. Dysmenorrhoea was mild and settled with simple analgesia.
On examination she appeared mildly pale but was otherwise well. Abdominal palpation revealed a firm mass corresponding to a twenty-week-size uterus, mildly tender and fixed to the pelvis. On speculum examination, the cervix was pushed high and to the right, lying against the upper lateral vaginal wall rather than centrally. Bedside ultrasound showed a bulky uterus of approximately 20cm in diameter with a cavity that could not be clearly identified, and a probable right ovarian endometrioma. Blood test showed mild anaemia and slightly elevated CA 125 and the rest were unremarkable.
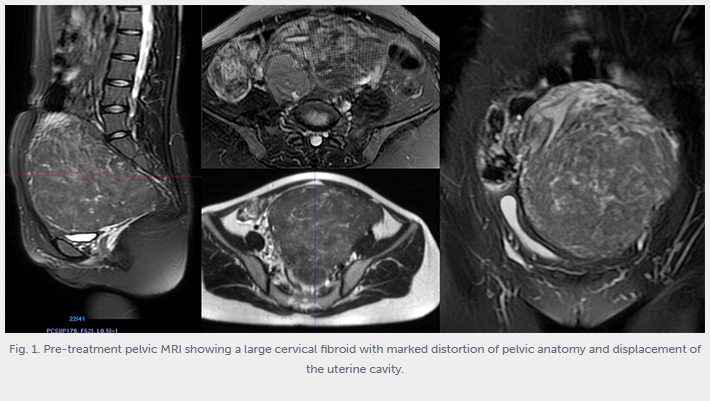
A 1.5T pelvic MRI with intravenous contrast clarified the picture. A solid, benign-appearing mass measuring 14.8 × 11.2 × 13cm, hypointense on both T1 and T2 sequences, was consistent with a fibroid (Figure 1). The mass pushed the cervical canal to the right, where it appeared elongated and stretched, and the uterine cavity was displaced superiorly and to the right. A 4cm right adnexal endometrioma was also noted. The reporting radiologist concluded that this was most likely a large cervical fibroid, with a differential of a left intramural fibroid extending into the cervix. This MRI appearance, where the cervix sits on top of a central pelvic mass, is classically described as the “lantern on the dome of St Paul’s” sign.5
The clinical picture was coherent. A young woman with primary infertility, deep dyspareunia, and a distorted uterine cavity sitting on top of a large cervical fibroid that had rearranged her pelvic anatomy.
Discussion
The first instinct in any unit is to operate. In Mrs PS’s case, that instinct deserved a second thought – uterine-preserving technique would be ideal.
A cervical fibroid of this size sits in arguably the most unforgiving corner of the pelvis. The ureters are typically displaced and splayed across the mass, and the uterine branches supplying it are dilated and high-flow. Published series on large cervical myomectomies consistently report high rates of intra-operative haemorrhage, bladder injury, and ureteric injury, often requiring preoperative ureteric stenting and, not infrequently, conversion to hysterectomy.1,2 In a 29-year-old with primary infertility, conversion to hysterectomy is not an acceptable option.
Cervical myomectomy, even when successful, brings its own problems. Reconstructing a cervix after enucleating a 14cm fibroid leaves a canal that is often scarred or shortened. This is not a minor point for a woman hoping to carry a pregnancy, and reports of subsequent cervical incompetence are well recognised.2
Medical therapy had little to offer here. Combined oral contraceptives and the levonorgestrel intrauterine system do not shrink fibroids of this size, and the distorted cavity would not accept a device. Dienogest treats her concurrent endometriosis but does not reduce fibroid bulk. GnRH analogues can achieve up to 30-50% volume reduction, but the effect is temporary and the fibroid regrows once therapy stops.4 More importantly, none of these options addresses her infertility within a realistic time frame. She had already waited four years.
This is where HIFU earns its place in the conversation. HIFU uses focused ultrasound beams delivered through an extracorporeal transducer to produce coagulative necrosis at a precise focal point inside the fibroid, without incision, without blood loss, and without disturbing the surrounding myometrium or endometrium.3,6 The biology is attractive in a fertility context. Because the endometrium and normal myometrium are preserved, there is no uterine scar to weaken future pregnancies. Meta-analyses now report pregnancy rates after HIFU that are comparable to myomectomy and clearly superior to uterine artery embolization, with lower rates of adhesions and ovarian compromise.3,7
HIFU is not a universal solution. Patient selection matters. Ideal candidates have an abdominal wall thickness under 4cm, fibroids within 13cm of the skin, and lesions that are hypointense on T2 imaging, which predict good energy absorption.6 Mrs PS met these criteria. Cervical location has traditionally been viewed with caution because of the theoretical risk of cervical stenosis from thermal injury, and this was discussed with her openly.
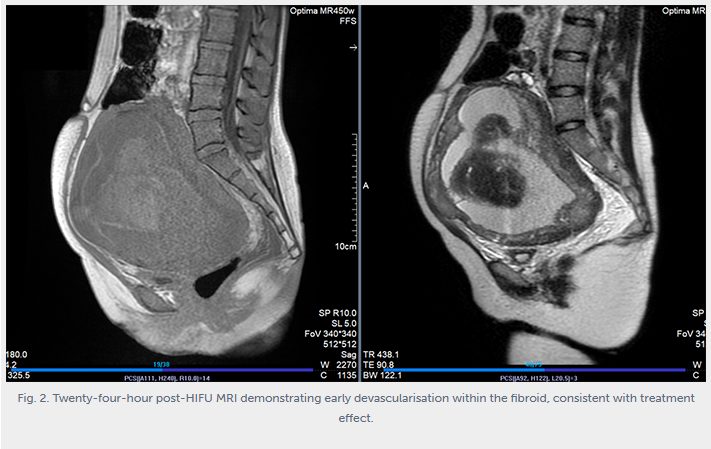
She underwent a single session of ultrasound-guided HIFU. Early post-treatment MRI at 24 hours demonstrated initial devascularisation of the fibroid (Figure 2).
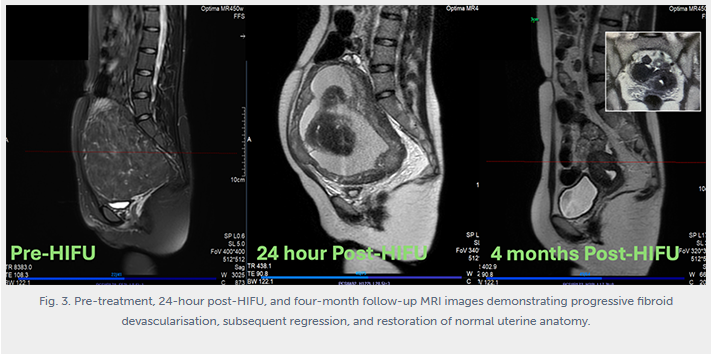
Follow-up MRI at four months showed a uterus returned to normal size, a normal-appearing endometrium, and a persistent small right endometrioma (Figure 3). Clinically, her abdominal girth had normalised, her dyspareunia had resolved, and her cervix had returned to a midline position. She was cleared to resume attempts at conception, with the understanding that any future pregnancy should be monitored and delivery planned with awareness of her treated uterus.3
What this case illustrates, more than anything, is that the best operation is sometimes no operation at all. A 14cm cervical fibroid in a young woman with infertility is not solved by picking the best surgical approach. It is solved by picking the approach that protects her fertility, preserves her anatomy, and avoids iatrogenic injury. In 2026, that increasingly means considering non-invasive ablative options before reaching for a scalpel.
Conclusions
- Cervical fibroids distort pelvic anatomy in predictable, dangerous ways. They displace ureters, stretch the cervical canal, and shift the uterine cavity. MRI should be standard before any intervention.
- Fertility preservation changes the risk calculation. In a young woman hoping to conceive, hysterectomy is not an option.
- Medical therapy rarely solves for large fibroid. Hormonal options may soften symptoms but do not deliver durable volume reduction for long term solution or address infertility.
- HIFU is a game changer for treating large fibroid or adenomyosis with minimal risks to the patients, preserving fertility, and has good success rate. For carefully selected patients, it offers a non-invasive, uterus-sparing alternative with increasingly robust pregnancy outcome data around the world. As we could see, the result of four-month follow-up MRI showed normal uterus with normal endometrium.
References:
- Sparic R, Mirkovic L, Malvasi A, Tinelli A. Epidemiology of uterine myomas: a review. Int J Fertil Steril. 2016;9(4):424–435.
- Ferrari F, Forte S, Valenti G, Ardighieri L, Barra F, Esposito V, et al. Current treatment options for cervical leiomyomas: a systematic review of literature. Medicina (Kaunas). 2021;57(2):92.
- Zhang G, Li L, Sun M, Yu X. Progress in high intensity focused ultrasound ablation for fertility preservation therapy of uterine fibroids and adenomyosis. Reprod Sci. 2024;31(12):3677–3688.
- Donnez J, Dolmans MM. Uterine fibroid management: from the present to the future. Hum Reprod Update. 2016;22(6):665–686.
- Yadav P, Singh PK, Kumar A. Cervical fibroid – a surgical quandary in gynecology. J Surg Case Rep. 2026;2026(3):rjae
- Cheung VYT. High-intensity focused ultrasound therapy. Best Pract Res Clin Obstet Gynaecol. 2018;46:74–83.
- Li Y, Yin L, Fang L, Xue M. HIFU as an alternative modality for patients with uterine fibroids who require fertility-sparing treatment. Int J Hyperthermia. 2022;39(1):1636–1644.